



Cardiovascular Outcomes Trials Answer Long-Asked Questions – But New Questions Arise
June 12, 2015 | Contributor: Eamonn O'Connor, Ph.D.
The recent American Diabetes Association’s 75th Scientific Sessions in Boston saw the release of data from the ELIXA cardiovascular outcomes trial (CVOT) for lixisenatide (Sanofi/Zealand Pharma’s Lyxumia), the first such trial completed for the GLP-1 receptor agonist drug class.
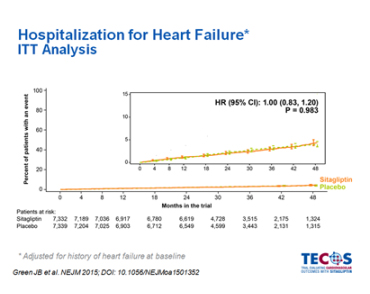
However, it was the publication of the data from the CVOT for sitagliptin (Merck’s Januvia/Ono’s Glactiv), known as TECOS1, that was most eagerly anticipated; this is because the previous CVOTs for saxagliptin (AstraZeneca’s Onglyza) and alogliptin (Takeda/Furiex’s Nesina/Vipidia) had raised significant concerns about a potential risk for increased rates of hospitalization due to heart failure. The results from TECOS therefore, were viewed as pivotal as to whether this risk was a feature specific to the DPP-IV inhibitor drug class.
To the relief of physicians, patients, and undoubtedly Merck, TECOS overwhelmingly proved that sitagliptin is safe for use in type 2 diabetes patients. As with the CVOTs for saxagliptin (SAVOR-TIMI 53 trial)2 and alogliptin (EXAMINE)3, TECOS assessed the use of sitagliptin in patients who had established cardiovascular disease (CVD), so the demonstrations of safety in this patient group at increased risk of CV events was widely welcomed. In particular, the lack of any signal in hospitalization for heart failure (see figure below), the outcome which raised questions over the safety of saxagliptin and alogliptin, was widely heralded.
The other CVOT to release data at the meeting was the ELIXA trial. The results from this study were also welcomed as they demonstrated the safety of lixisenatide with regards to CV outcomes. One particular aspect of this trial intrigued me, however. Despite all efforts to minimize differences in glycemic control between the lixisenatide and placebo groups, a significant difference emerged, with the lixisenatide-treated patients demonstrating a 0.27% greater reduction in HbA1c than the placebo group. For me, reasons for this difference should be addressed. Is it a consequence of using GLP-1 receptor agonist as a therapy, something that was denied to the placebo group? Widely acknowledged as the most effective glucose-lowering agents available outside of insulins, did the use of a GLP-1 receptor agonist result in better glycemic outcomes? Or alternatively, did the investigators fail to provide adequate antidiabetic therapy to the placebo group? While glycemic control was not an endpoint of the trial; the possibility remains that the greater reduction in HbA1c in the lixisenatide-treated patients may reflect better treatment practices in these patients. If this is the case, it is not a stretch to suggest that inferior treatment practices in the placebo group would therefore have influenced the CV endpoints in the trial.
Undoubtedly, both physicians and patients will be reassured by the results of both TECOS and ELIXA, ensuring that use of these agents poses no additional CV risk to patients. But as results from these and other CVOTs emerge in the coming months and years, more questions will undoubtedly surface. Despite this, the belief remains that we are better placed to answer them than ever before.
Eamonn O'Connor, Ph.D., is a business insights analyst on the Cardiovascular, Metabolic, and Renal Disorders team at Decision Resources Group.